
The best way to ensure the process of progressing pull-ups goes smoothly is to assess and address mobility issues first. Joint mobility is the degree to which an articulation (where two bones meet) is allowed to move before being restricted by surrounding tissues (ligaments/tendons/muscles etc.), otherwise known as the range of uninhibited movement around a joint.
For those clients who want to learn how to do pull-ups, gaining a sense of how well their shoulder can move before working on strength gains will more likely guarantee success. We all know the shoulder is a complicated joint! Taking this into account and breaking down the different joint actions and potential restrictions that contribute to pull-up performance is a helpful place to start before assessing mobility.
There are three joint actions/areas in which mobility will affect the ability to produce an ideal pull-up:
1) Thoracic spine mobility coupled with latissimus dorsi length
2) Scapular upward/downward rotation
3) Glenohumeral internal/external rotation
If there is a breakdown in mobility or muscle imbalances are present, they are more likely to follow the progression above. If the thoracic spine is restricted and lats short, this will, in turn, prevent proper scapular rotation. If the scapulae are unable to function optimally, then the rotator cuff musculature and larger, global internal rotators will become imbalanced as well.
Thoracic Mobility Assessment
While latissimus dorsi can be short and overactive without limited thoracic mobility, limited thoracic mobility almost always occurs with short lats. A common compensatory pattern of shortened, overactive lats and/or a hyperkyphotic thoracic spine that occurs during a pull-down is bent elbows and a rounded back (and often forward head) during the start of the exercise and an even more rounded spine, lending to anterior/superior pointing humeral heads at the bottom of the exercise. Explore how to fully assess thoracic mobility.


Scapular Upward/Downward Rotation and “Tipping” Assessment
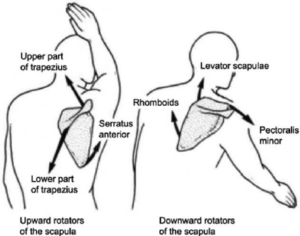
Upward rotation occurs when the arm abducts and the inferior border of the scapula rotates laterally-superiorly over the rib cage. When the arm adducts, the scapula downwardly rotates to return to its resting position.
One common dysfunction is when the muscles that perform downward rotation, the levator scapulae, rhomboids and pec minor, become short and overactive, thereby restricting upward rotation.
Also common is scapular “winging”, where the inferior/medial border of the scapulae pop out, either statically or during movement. This is an indication of weak serratus anterior and lower trapezius, and overactive levator scapulae and pec minor. There is definitely overlap with these two dysfunctions. Learn how to do a full assessment of these maladaptive patterns of scapular rotation dysfunction.
Humeral External Rotation ROM Assessment
Most times when thoracic mobility is limited and scapular function sub-optimal, it is likely that the muscles of the rotator cuff are imbalanced. Expect the internal rotators such as subscapularis, teres major and pec major to be short and overactive. Concordantly, the smaller external rotator muscles infraspinatus and teres minor are likely to be long and weak.
Strengthening the infraspinatus and teres minor after releasing and lengthening the internal rotators will ensure a more mobile and efficient shoulder joint, prepared to take on pull-up progressions. Assessing humeral external rotation will be the last step before programming mobility drills into your clients’ pull-up progression program.


